You are here
Position Statement 33: Substance Use Disorders
Policy
Substance use disorders are recognized as primary, progressive, chronic, relapsing and treatable diseases, as detailed in the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), with extensive evidence-based treatment principles and protocols. Taking advantage of the brain’s marvelous plasticity, addictions literally remold the brain’s circuitry to assign supreme value to our compulsions, ignoring health, work, family, and life itself. These conditions have a dramatic impact on the lives of individuals, their families and partners, and society as a whole, throughout the lifespan.
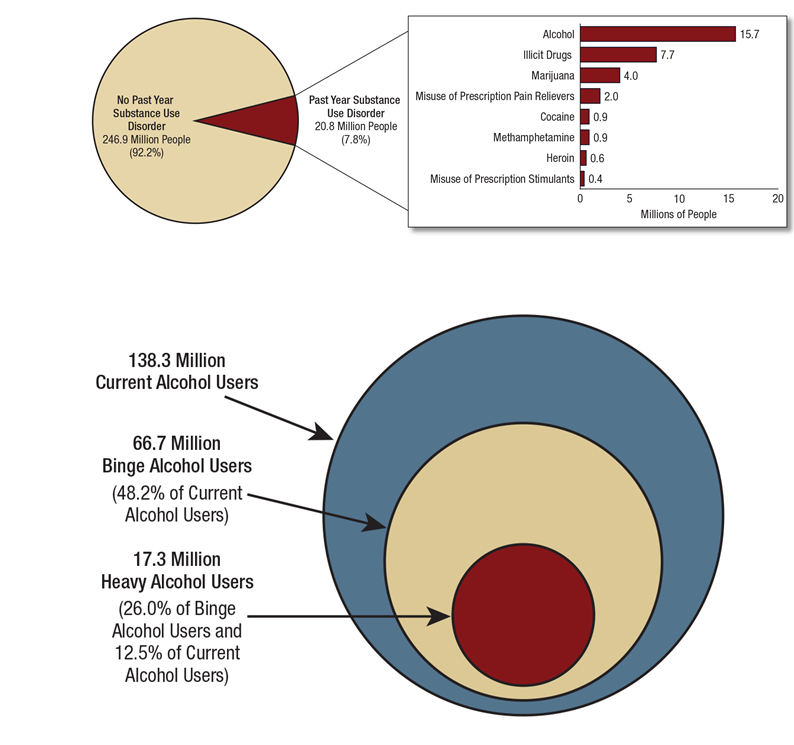
There is a substantial relationship between mental health and substance use disorders, and many people are subject to both. The 2017 analysis of the National Epidemiological Survey on Alcohol and Related Conditions (NESARC)[i] revealed that of adults reporting “alcohol dependence” (as defined in the DSM-4), 54% had experienced an anxiety disorder in their lifetime and 34% had experienced a personality disorder in their lifetime. According to the 2016 Surgeon General’s report on substance use disorders, “…of the 20.8 million people aged 12 or older who had a substance use disorder during the past year, about 2.7 million (13 percent) had both an alcohol use and an illicit drug use disorder, and 41.2 percent also had a mental illness. Particularly striking is the …high prevalence of co-existing alcohol use disorder in those meeting criteria for PTSD. It is estimated that 30-60 percent of patients seeking treatment for alcohol use disorder meet criteria for PTSD and approximately one third of individuals who have experienced PTSD have also experienced alcohol dependence at some point in their lives.”[ii] According to SAMHSA’s 2014 National Survey on Drug Use and Health (NSDUH), approximately 7.9 million adults had co-occurring disorders in 2014. During the past year, for those adults surveyed who experienced substance use disorders and any mental illness, rates were highest among adults ages 26 to 49 (42.7%). For adults with past-year serious mental illness and co-occurring substance use disorders, rates were highest among those ages 18 to 25 (35.3%) in 2014.[iii]
Mental Health America (MHA) advocates complete integration of the treatment of substance use and mental health disorders and an end to invidious discrimination against people in recovery from substance use disorders. Integrating all behavioral health treatment with other health treatment should also be the goal. This will require changes in practice, in training of practitioners, and in the legal treatment of substance use treatment data – including conforming the archaic 42 CFR Part 2 (which limits access to substance use treatment information) to HIPAA. Early identification of both substance use and mental health disorders should be followed by early treatment, without regard for administrative systems and funding silos. Prevention of disorders and promotion of health and wellness also should be fully integrated. Throughout this position statement, MHA seeks to raise the issue of parity of treatment for the substance use and mental health aspects of each issue addressed, even when the preceding literature has emphasized one or the other.
Background
In 2004, the World Health Organization published a report entitled "Neuroscience of Psychoactive Substance Use and Dependence."[iv] The Report Summary underscored the following points:
- There is a need to increase public awareness regarding the complex nature of the problems and the biological processes underlying drug dependence.
- "...with recent advances in neuroscience, it is clear that substance dependence is a disorder of the brain as any other neurological or psychiatric illness."
- "Substance dependence is a chronic, relapsing disorder with a biological and genetic basis, and is not simply due to a lack of will or desire to quit."
- The greatest barrier to integrated treatment is the "silo" mentality - the fragmentation of mental health and substance use treatment services.[v]
The Surgeon General’s 2016 Report, Facing Addiction in America,[vi] sounded the clarion call:
Now is the time for this Report. The substance misuse problem in America won’t wait. Almost 22.5 million people reported use of an illegal drug in the prior year. Over 20 million people have substance use disorders, and 12.5 million Americans reported misusing prescription pain relievers in the past year. Seventy-eight people die every day in the United States from an opioid overdose, and those numbers have nearly quadrupled since 1999. Despite the fact that we have treatments we know are effective, only one in five people who currently need treatment for opioid use disorders is actually receiving it.[vii]
We now understand much better why substance use disorders are so hard to treat. As use becomes an ingrained behavior, impulsivity shifts to compulsivity, and the primary drivers of repeated substance use shift from positive reinforcement (feeling pleasure) to negative reinforcement (feeling relief), as the person seeks to stop the negative feelings and physical illness that accompany withdrawal. Eventually, the person begins taking the substance not to get “high,” but rather to escape the “low” feelings to which, ironically, chronic drug use has contributed. Compulsive substance seeking is a key characteristic of addiction, as is the loss of control over use. Compulsivity helps to explain why many people with addiction experience relapse after attempting to abstain from or reduce use.
Thus, MHA advocates for comprehensive wellness, prevention, early identification, treatment, and supportive services for substance use disorders, which will require a major new investment of public resources. The so-called “opioid epidemic,” fueled by the rapid and widespread deindustrialization and social disruption of American society at the turn of the century as well as the over prescription and cheap availability of powerful prescription pain drugs and new generations of designer drugs, has finally caught the imagination of the American electorate. MHA intends to harness this political moment to promote more effective and more integrated treatment of substance use and mental health conditions.
The DSM-5 no longer uses the terms “substance abuse” and “substance dependence.” Rather, it refers to “substance use disorders,” which are defined as mild, moderate, or severe based on the number of diagnostic criteria met by the person. Substance use disorders occur when the recurrent use of alcohol or other drugs causes clinically and functionally significant impairment, such as health problems, disability, and failure to meet major life responsibilities.
DSM-5 Criteria for Diagnosing Substance Use Disorders
|
|
|
|
|
|
|
|
|
|
|
|
SAMHSA and the DSM-5 recognize nine distinct addictive disorders:[viii]
Alcohol use disorder is still the most common form of substance use disorder in America, fueled by widespread legal access and social approval of moderate drinking. Many Americans begin drinking at an early age. In 2012, about 24% of eighth graders and 64% of twelfth graders used alcohol in the past year.
Excessive alcohol use can increase a person’s risk of developing serious health problems in addition to the issues associated with intoxication behaviors and alcohol withdrawal symptoms. According to SAMHSA, an estimated 17 million people have an alcohol use disorder. According to the Centers for Disease Control and Prevention (CDC), excessive alcohol use causes 88,000 deaths a year.
The definitions for the different levels of drinking include the following:
- Moderate Drinking—According to the Dietary Guidelines for Americans, moderate drinking is up to 1 drink per day for women and up to 2 drinks per day for men.
- Binge Drinking—SAMHSA defines binge drinking as 5 or more alcoholic drinks on the same occasion on at least 1 day in the past 30 days. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) defines binge drinking as a pattern of drinking that produces blood alcohol concentrations (BAC) of greater than 0.08 g/dL. This usually occurs after 4 drinks for women and 5 drinks for men over a 2 hour period.
- Heavy Drinking—SAMHSA defines heavy drinking as drinking 5 or more drinks on the same occasion on each of 5 or more days in the past 30 days.
Excessive drinking puts a person at risk of developing an alcohol use disorder in addition to other health and safety problems. Genetics have also been shown to be a risk factor for the development of an alcohol use disorder.
Tobacco Use Disorder
According to the CDC, more than 480,000 deaths each year are caused by cigarette smoking. Tobacco use and smoking do damage to nearly every organ in the human body, often leading to lung cancer, respiratory disorders, heart disease, stroke, and other illnesses.
In 2014, an estimated 66.9 million Americans aged 12 or older were current users of a tobacco product (25.2%). Young adults aged 18 to 25 had the highest rate of current use of a tobacco product (35%), followed by adults aged 26 or older (25.8%), and by youths aged 12 to 17 (7%).
In 2014, the prevalence of current use of a tobacco product was 37.8% for American Indians or Alaska Natives, 27.6% for whites, 26.6% for blacks, 30.6% for Native Hawaiians or other Pacific Islanders, 18.8% for Hispanics, and 10.2% for Asians.
Adults with mental health or substance use disorders smoke cigarettes more than adults without these disorders. Approximately 25% of adults in the U.S. have some form of mental illness or substance use disorder, and these adults consume almost 40% of all cigarettes smoked by adults.[ix] According to the National Institute on Drug Abuse, the rate of smoking in patients with schizophrenia has ranged as high as 90 percent in clinical samples.[x]
Opioid Use Disorder
Opioids reduce the perception of pain but can also produce drowsiness, mental confusion, euphoria, nausea, constipation, and, depending upon the amount of drug taken, can depress respiration. Illegal opioid drugs and legally available pain relievers such as codeine, oxycodone and hydrocodone and tramadol products can cause serious health effects in those who misuse them. Some people experience a euphoric response to opioid medications, and it is common that people misusing opioids try to intensify their experience by snorting or injecting them. These methods increase their risk for serious medical complications, including overdose. Other users have switched from prescription opiates to heroin or black-market fentanyl (commonly used for anesthesia but rarely if ever prescribed for any other legitimate medical use) as a result of appropriate but more restrictive opioid prescribing guidelines, availability and lower price. Because of variable purity and other chemicals and drugs mixed with heroin on the black market, this also increases risk of overdose. Overdoses with opioid pharmaceuticals led to almost 17,000 deaths in 2011. Since 1999, opiate overdose deaths have increased 265% among men and 400% among women.
In 2014, an estimated 1.9 million people had an opioid use disorder related to prescription pain relievers and an estimated 586,000 had an opioid use disorder related to heroin use. In 2015, the Centers for Disease Control and Prevention reported 33.092 total opioid overdose deaths – 16 percent more than the previous record, set the year before.
Symptoms of opioid use disorders include strong desire for opioids, inability to control or reduce use, continued use despite interference with major obligations or social functioning, use of larger amounts over time, development of tolerance, spending a great deal of time to obtain and use opioids, and withdrawal symptoms that occur after stopping or reducing use, such as negative mood, nausea or vomiting, muscle aches, diarrhea, fever, and insomnia.
Because opioids are commonly prescribed for pain, and many people begin using them in that way, it is critical that prescribing practices and medical counselling be radically changed to minimize the potential for addiction that has now begun to be understood.
Cannabis Use Disorder
Marijuana is the most-used drug after alcohol and tobacco in the United States. According to SAMHSA data, in the past year, 4.2 million people ages 12 and up met criteria for a substance use disorder based on marijuana use.
Marijuana’s immediate effects include distorted perception, difficulty with thinking and problem solving, and loss of motor coordination. Long-term use of the drug can contribute to respiratory infection, impaired memory, and exposure to cancer-causing compounds. Heavy marijuana use in youth has also been linked to increased risk for developing mental illness and poorer cognitive functioning.
Some symptoms of cannabis use disorder include disruptions in functioning due to cannabis use, the development of tolerance, cravings for cannabis, and the development of withdrawal symptoms, such as the inability to sleep, restlessness, nervousness, anger, or depression within a week of ceasing heavy use. Cannabis use can be particularly damaging to young people.[xi] On the other hand, more controlled cannabis use is a promising practice as a substitute for opioids in treating pain, and studies of cannabis may yield formulations and protocols that increase its utility and decrease the potential for physical damage to the lungs and airways and addiction.
Stimulant Use Disorder
Stimulants increase alertness, attention, and energy, as well as elevate blood pressure, heart rate, and respiration. They include a wide range of drugs that have historically been used to treat conditions, such as obesity, attention deficit hyperactivity disorder and, occasionally, depression. Like other prescription medications, stimulants can be diverted for illegal use. The most commonly abused stimulants are amphetamines, methamphetamine, and cocaine. But dextroamphetamine, and phentermine products; mazindol products; and methylphenidate or dexmethylphenidate products are used as well. According to the DSM, caffeine doesn’t count, though its addictive effects are conceded. Stimulants can be synthetic (such as amphetamines) or can be plant-derived (such as cocaine). They are usually taken orally, snorted, or injected intravenously.
In 2014, an estimated 913,000 people ages 12 and older had a stimulant use disorder because of cocaine use, and an estimated 476,000 people had a stimulant use disorder as a result of using other stimulants besides methamphetamines. In 2014, almost 569,000 people in the United States ages 12 and up reported using methamphetamines in the past month.
Symptoms of stimulant use disorders include craving for stimulants, failure to control use when attempted, continued use despite interference with major obligations or social functioning, use of larger amounts over time, development of tolerance, spending a great deal of time to obtain and use stimulants, and withdrawal symptoms that occur after stopping or reducing use, including fatigue, vivid and unpleasant dreams, sleep problems, increased appetite, or irregular problems in controlling movement.
Hallucinogen Use Disorder
Hallucinogens including LSD, PCP, ketamine, ecstasy (MDMA), peyote, mescaline, and psilocybin can be chemically synthesized (as with lysergic acid diethylamide or LSD) or may occur naturally (as with psilocybin mushrooms). These drugs can produce visual and auditory hallucinations, feelings of detachment from one’s environment and oneself, and distortions in time and perception.
In 2014, approximately 246,000 Americans had a hallucinogen use disorder. Symptoms of hallucinogen use disorder include craving for hallucinogens, failure to control use when attempted, continued use despite interference with major obligations or social functioning, use of larger amounts over time, use in risky situations like driving, development of tolerance, and spending excessive time and energy to obtain and use hallucinogens.
As with cannabis, recent studies have shown promise in using MDMA, psilocybin, and LSD to treat depression, PTSD, and alcohol and tobacco use disorders.[xii] Researchers are also looking at legal but widely abused drugs like ketamine, an anesthetic that also can produce hallucinations. The FDA recently put the ketamine-based drug esketamine on the fast track for approval as a treatment for major depression.[xiii] While recognizing the addictive dangers of these drugs, it is important to explore the therapeutic possibilities of psychoactive substances in controlled, randomized trials.
Sedatives, Hypnotics (“sleeping pills”), Anxiolytics (tranquilizers), and Cough and Cold Medication
The DSM-5 categorizes these substances together, giving barbiturates, benzodiazepines (such as Valium and Xanax), and benzodiazepine hypnotics (such as Rohypnol or “roofies”) as examples. Meprobamate products and muscle relaxants are in the same class of potential use disorder. While these medications can all be useful over a short course of treatment to alleviate anxiety and insomnia, their long-term effects are similar to opioids, and they should be prescribed with the same care. Over-the-counter cough and cold medicines are similarly subject to overuse, causing intoxication.
Inhalant Use Disorder
Paint thinners, glue and aerosol spray can all produce a “high,” often at the cost of permanent brain damage. Other inhalants, including cleaning fluids, gasoline and lighter gases, anesthetics, solvents, and spray paint, can also produce significant effects on the body. These are extremely dangerous chemicals, and “huffing” them through the nose or mouth over any period of time can produce dementia-like organic brain defects, violent mood swings, and acting out in ways that sometimes requires institutionalization. There is no known treatment for these tragic effects.
Behavioral Addictions
Gambling disorder is specifically covered by the DSM-5, and there is a whole chapter on sexual dysfunctions, which focuses on sexual impairment but neglects excessive sexual activity and pornography addiction – “sexaholism”, as encountered in 12-step groups like Sex Addicts Anonymous, http://www.recovery.org/topics/about-the-sex-addicts-anonymous-12-step-recovery-program/. Video game addiction is not discussed at all, but seductive graphics and sound experiences, smart phones, enhanced speakers and video monitors and fast internet can produce compulsive, ungovernable urges in some people, which are at the core of the experience of addiction in the brain. Smartphones, junk food (especially products with large amounts of refined sugars), and shopping can also be compulsive or addictive.
Prevalence
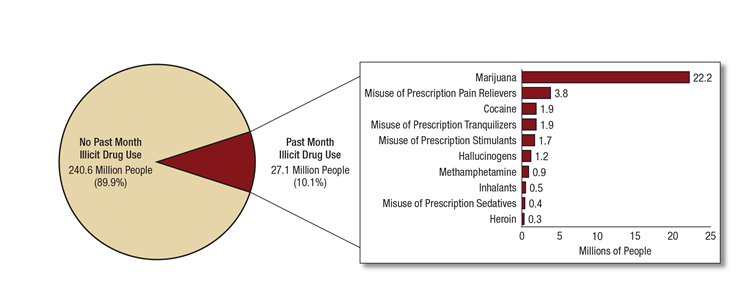
Substance use disorders are extraordinarily prevalent in American society, but only about 10% of people in need get treatment. The Surgeon General estimated that 175 million persons aged 12 and older (65.7 percent of this population) reported alcohol use in the past year, with over 66 million (24.9 percent) reporting binge drinking in the past month. More than 36 million (13.5 percent) reported using marijuana in the past year, 12.5 million reported misusing prescription pain relievers, and over 300,000 reported using heroin in the past year. Almost 8 percent of the population met diagnostic criteria for a substance use disorder for alcohol or illicit drugs, and another 1 percent met diagnostic criteria for both an alcohol and illicit drug use disorder. Although 20.8 million people (7.8 percent of the population) met the diagnostic criteria for a substance use disorder in 2015, only 2.2 million individuals (10.4 percent) received any type of treatment. Of those treated, 63.7 percent received treatment in specialty substance use disorder treatment programs.[xiv] The following tables summarize the prevalence of use disorders for alcohol and illicit drugs.[xv]
Treatment
The Surgeon General’s 2016 Report, Facing Addiction in America, supra, did not catalogue the options that are now available, which will be discussed here. Treatment programs, peer support programs, and self-help organizations provide an array of recovery supports for substance use disorders. William White's seminal work, Slaying the Dragon: The History of Addiction Treatment and Recovery in America,[1] is an important resource to gain an understanding of the insights into and treatments of substance use disorders that have been developed and popularized in America.
History of Alcohol Use Disorder Treatment
The concept of alcoholism as a disease has been understood at least since Benjamin Rush, the Surgeon General of George Washington’s revolutionary armies, first laid out the case in a pamphlet dated 1784. Rush was also one of the first to prescribe total abstinence from spirits as the sole remedy.
The first American mutual self-help movement was the Washingtonians, started in 1840. The movement was an immediate success. At its peak, it reached many hundreds of thousands. They went to taverns to recruit. Washingtonians, or most of them, “believed that social camaraderie was sufficient to sustain sobriety and that a religious component would only discourage drinkers from joining.”
The Washingtonians were hugely important in shaping future self-help movements. It was they who introduced sharing of experiences, in lieu of making abstract speeches. It was they who first held closed, alcoholics-only meetings. It was they who first enlisted the reformed drunkard as missionary to the drinker, pioneering the concept of service as a tool of self-recovery. They sustained members’ sobriety through regular weekly fellowship meetings, encouraged all manner of sober recreation, involved women and other family members in their process, and founded some of the first “homes” where drunkards could go to dry out and live in sober communities. But their disorganization led to their demise, and to the rise of more and more militant and moralistic temperance movements, culminating in the Anti-Saloon League, the Women’s Christian Temperance Union and, in 1920, Prohibition.
Prior to Prohibition, other self-help organizations came and went, as did sanatoria, asylums, farms, homes, colonies and other institutions for dipsomaniacs. White traces the bad blood that sometimes exists today between the addiction field and psychiatry back to early institutional conflict. Heads of the insane asylums did not want to have inebriates there, because it would damage the reputation of their facilities. Heads of inebriate treatment facilities equally did not want to send inebriates to the early insane asylums, where free and liberal use of whiskey, opium and other drugs, both among patients and staff, were more the rule than the exception.
Soon after the end of Prohibition in 1933, Alcoholics Anonymous (AA) was born. AA supported the proposition that an alcoholic is unable to control his or her drinking and recovery is possible only with total abstinence and peer support. Alcoholics constituted a special group who are unable to control their drinking from birth. Initially, AA described this as "an allergy to alcohol."
Although AA was instrumental in emphasizing the "disease concept" of alcoholism, the defining work was done by Elvin Jellinek, M.D., of the Yale Center of Alcohol Studies. In his book, The Disease Concept of Alcoholism, published in 1960,[ii] Jellinek described alcoholics as individuals with tolerance, withdrawal symptoms, and either "loss of control" or "inability to abstain" from alcohol. He asserted that these individuals could not drink in moderation, and, with continued drinking, the disease was progressive and life-threatening.[iii]
It seems clear that AA has helped many people overcome alcohol use disorders. However, few would describe alcohol addiction as different in kind from habituation to use of opiates and other substances, and it is not at all clear that total abstinence and peer support combined with the religious focus of AA are either necessary or sufficient to address substance use disabilities. As stated succinctly by Gabrielle Glazer in the Atlantic, “The history of AA is the story of how one approach to treatment took root before other options existed, inscribing itself on the national consciousness and crowding out dozens of newer methods that have since been shown to work better.”[iv]
In 1970, in response to growing advocacy among service providers and legal advocates for increased confidentiality to combat stigma against people living with alcohol use and other substance use disorders, the federal government enacted the rule codified at 42 CFR Part 2, which sought to protect information about these disorders from falling into the hands of employers, police, and others, who might use the information to fire or arrest people. This rule codified the anonymity that is central to the AA approach to alcohol use disorder treatment. But it failed to take account of the need to treat alcohol use disorder in tandem with other health conditions. 42 CFR Part 2 was not conformed to HIPAA when HIPAA was enacted in 1996, and because of this stands today as an impediment to the integration of health record information and to the integration of general and behavioral health care.
Comparative Effectiveness of Alcohol Use Disorder Treatments
A meticulous analysis of treatments, published more than 15 years ago in The Handbook of Alcoholism Treatment Approaches but still considered one of the most comprehensive comparisons, ranks AA 38th out of 48 methods.[v] Rank ordered, the evidence is strongest for:
1. Receiving honest but non-confrontational one-on-one feedback regarding one’s alcohol- related health from a health professional;
2. Non-confrontational strategic Motivational Interviewing;
3. The medication acamprosate (see below);
4. A complex set of cognitive and behavioral methods called the Community Reinforcement Approach
5. The assigning of a Self-Change Manual, also called Bibliotherapy
6. The medication naltrexone (see below);
7. Behavioral Self-Control Training (a moderation approach);
8. Behavioral Contracting for rewards given in exchange for clean drug test results:
9. Social Skills Training
10. Behavioral Marital Therapy
A common theme in all of these treatments is that they are delivered with empathy and without confrontation.
Of the 48 approaches ranked, the evidence is weakest for:
48. Educational tapes, lectures and films, upon which much time is spent in some rehabs;
47. General Alcoholism Counseling;
46. Psychotherapy;
45. Confrontational Counseling;
44. Relaxation Training;
43. Videotape Self-Confrontation or watching oneself behaving badly while intoxicated;
42-39.These four include three medications and Milieu Therapy;
38. Alcoholics Anonymous
According to a 2014 book by Lance and Zachary Dodes, the former a retired Harvard Medical School assistant clinical professor of psychiatry: “Peer reviewed studies peg the success rate of AA somewhere between five and 10 percent…. About one of every 15 people who enter these programs is able to become and stay sober.”[vi]
This contrasts with AA’s self-reported figures: A 2007 internal survey found that 33 percent of members said they had been sober for more than a decade. Twelve percent claimed sobriety for five to 10 years, 24 percent were sober for one to five years, and 31 percent were sober for under a year. Of course, those don’t take into account the large number of people who never make it through their first year of meetings, subsequently never completing the 12 steps (the definition of success, by AA’s standards).
Comparing AA to other treatments, a 2006 Cochrane Collaboration study concluded that its effectiveness is not scientifically established:
No experimental studies unequivocally demonstrated the effectiveness of AA or [12-step] approaches for reducing alcohol dependence or problems.
AA may help patients to accept treatment and keep patients in treatment more than alternative treatments, though the evidence for this is from one small study that combined AA with other interventions and should not be regarded as conclusive. Other studies reported similar retention rates regardless of treatment group. Three studies compared AA combined with other interventions against other treatments and found few differences in the amount of drinks and percentage of drinking days. Severity of addiction and drinking consequence did not seem to be differentially influenced by [AA] versus comparison treatment interventions, and no conclusive differences in treatment dropout rates were reported.[vii]
While AA has stimulated hope and recovery for many people, it is not for everyone, and its one-size-fits-all message of lifelong abstinence may serve as a barrier to seeking treatment. As Glazer concluded, “Whereas AA teaches that alcoholism is a progressive disease that follows an inevitable trajectory, data from a federally funded survey called the National Epidemiological Survey on Alcohol and Related Conditions show that nearly one-fifth of those who have had alcohol dependence go on to drink at low-risk levels with no symptoms of abuse.[viii] And a recent survey of nearly 140,000 adults by the Centers for Disease Control and Prevention found that nine out of 10 heavy drinkers are not dependent on alcohol and, with the help of a medical professional’s brief intervention, can change unhealthy habits.”
Medication-Assisted Treatment (MAT)
There are many different medications that are prescribed to treat two major drugs of addiction: opioids and alcohol. There are currently no FDA-approved medications used to treat other types of drug addiction, such as methamphetamine, marijuana, or cocaine dependence. There are many medications and over-the-counter remedies for tobacco use disorder, ranging from antidepressants to nicotine chewing gum, all of which cannot be listed here. The antidepressant bupropion was approved by the FDA in 1997 to help people stop smoking and is marketed as Zyban. Varenicline tartrate (Chantix) is a medication that has received FDA approval for smoking cessation. This medication, which acts at the sites in the brain affected by nicotine, may help people quit by easing withdrawal symptoms and blocking the effects of nicotine if people resume smoking
Addiction and the recovery process are commonly marked by strong cravings even after successful completion of detox and treatment. These cravings, a normal occurrence for those struggling to get and stay clean, can interfere with treatment and increase the risk of relapse. Fortunately, certain medications have proven very successful in helping to stave off these cravings and promoting abstinence. However, it should be noted that psycho-social support and talk therapy, as well as residential therapy when needed, are essential adjuncts to medication-assisted treatment. And 12-step programs, including AA, can be used to supplement medication-assisted treatment.
As stated by the New York Times in a September 30, 2017 editorial: “Multiple studies suggest medications help guard against relapse as well as addiction-related medical problems, allowing people to return to work and rebuild their lives. Yet fewer than a third of conventional drug treatment centers in the United States take this approach.”[ix]
MHA CANNOT OFFER MEDICAL ADVICE, AND NO ONE SHOULD BEGIN OR CURTAIL MEDICATION WITHOUT THE ADVICE OF A PHYSICIAN CONCERNING THE PERSON’S MEDICAL CONDITION AND POTENTIAL SIDE EFFECTS AND DRUG INTERACTIONS. THIS IS PARTICULARLY IMPORTANT FOR PEOPLE BEING TREATED FOR CO-OCCURRING MENTAL HEALTH CONDITIONS.
That said, the Surgeon General’s 2016 report does not inventory the most commonly prescribed drugs used for the treatment of opioid or alcohol dependence, which are:[x]
Buprenorphine
Buprenorphine, which is a partial opioid agonist, is used to treat someone who is addicted to an opioid – whether the substance being abused is heroin or a prescription painkiller, such as OxyContin or Vicodin. Of the few medications used for opioid dependence, buprenorphine is the first that can be prescribed for and obtained directly from the doctor’s office. Now, Neltrexone can as well. To date, other drugs used to treat opioid dependency – such as methadone – can only be administered in clinics.
Buprenorphine alone has potential for abuse and prescription diversion due to its opioid effects. However, formulations that contain a combination of buprenorphine and naloxone decrease the potential for abuse because naloxone otherwise blocks a robust opioid effect and, further, will initiate withdrawal symptoms if attempts are made to misuse it via injection.
When used properly, these buprenorphine-containing medications can both alleviate unpleasant opioid withdrawal and decrease associated cravings.
These medications are also difficult to overdose on, due to the ceiling effect that buprenorphine has (and to the opioid antagonism of naloxone, in the combination formulations). Once you reach a certain dose, the effects plateau and don’t increase with higher doses.
Probuphine
In May 2016, the FDA approved the first buprenorphine implant designed to treat opioid dependence. Like methadone and naltrexone, Probuphine is designed to help individuals recover from an opioid addiction by alleviating cravings and withdrawal symptoms without creating a euphoric high. By stabilizing the patient and reducing the sometimes overwhelming cravings associated with opioid addiction, the individual is better able to engage in treatment and therapy.
The Probuphine implant is made of four rods that are inserted into the upper arm. The rods administer a continuous dose of buprenorphine into the bloodstream for a treatment period of 6 months—making it a convenient alternative to the other forms of buprenorphine (daily pills and dissolvable films). The drug is prescribed to patients who are currently stable on low-to-moderate doses of buprenorphine. Probuphine is not recommended beyond two 6-month treatment periods.
This medication presents advantages over other maintenance medications like methadone. Specifically:
- Probuphine does not require daily administration, as it releases a low dose of the drug on a continuous basis.
- Probuphine cannot be abused if the implant stays in place.
Methadone
Methadone is a full opioid agonist, which means that it produces similar effects to other opioids. However, because it is longer-acting than drugs like heroin, the effects are milder and shouldn’t significantly impact the individual’s ability to function.
Methadone is used to alleviate withdrawal symptoms and drug cravings in those addicted to heroin or painkillers. In fact, one dose can prevent cravings and withdrawal for up to a day and a half, according to the Center for Substance Abuse Treatment (CSAT). In order to prevent abuse, methadone is administered in a clinic on a set schedule.
Despite its relatively mild effects (no extreme highs), those taking methadone would likely still experience unpleasant withdrawal symptoms if methadone therapy were to suddenly stop.
Naloxone
Naloxone is an opioid antagonist, which means that it blocks the activity of opioids at the receptor sites – potentially reversing or preventing life-threatening overdoses. A naloxone injection may be administered in a medical emergency to those who are experiencing an opioid overdose. As a potentially life-saving intervention, both opioid users and family members should understand how naloxone works and how to use it in the event of an overdose.
Naloxone can be delivered by injection, nasal inhalant or in automatic injection devices, which are sometimes handed out as a harm reduction measure in communities hit hard by heroin abuse. Automatic naloxone injection devices have voice control and walk the injector through administration in a step-by-step manner.
Naltrexone
Naltrexone, which can come in an injectable or pill form, is used to treat patients who suffer from an addiction to alcohol or opioids. The injectable version is called Vivitrol. It may be administered intramuscularly, and therefore only requires monthly dosing. Oral dosing occurs once a day. Unlike buprenorphine and methadone, naltrexone lacks potential for diversion and abuse because it is not an opioid medication.
Naltrexone works by blocking the opioid receptors. What this means is that if you take the drug and then take alcohol or opioids, you won’t experience the usual euphoria or “high” associated with those substances. It may also decrease the general urge to use opioids or alcohol.
It’s important to note that naltrexone returns the person to being opioid naïve and as a result tolerance to opioids is decreased, so relapse can potentially be dangerous if the person returns to taking the amount previously used. Overdose and fatal respiratory depression may result.
Conversely, there aren’t any risks associated with drinking while taking the appropriate amount of naltrexone. While naltrexone blocks the individual from experiencing fully the rewarding effects of alcohol, it does not decrease the other intoxicating effects, such as impaired judgment and coordination.
Disulfiram
Disulfiram (Antabuse) helps to curb drinking behaviors by eliciting unpleasant effects when alcohol is consumed, discouraging the desire to drink. The unwanted effects, which appear about 10 to 30 minutes after alcohol consumption, include:
Sweating. Vomiting. Chest pain. Headache. Flushing. Anxiety. Blurred vision. Weakness. Heart palpitations. Vertigo. Confusion. Tachycardia.
The effects last for about an hour and are meant to deter the individual from engaging in drinking behavior. The severity of these reactions is thought to be related to the dose of disulfiram the patient takes and the amount of alcohol consumed.
Acamprosate
Acamprosate (Campral) is another medication used to prevent relapse and promote abstinence in those who are dependent on alcohol. According to the Center for Substance Abuse Treatment, when the brain becomes used to the presence of alcohol, a new “equilibrium” is set and maintained only when alcohol is present in the system. When alcohol use suddenly slows or stops altogether, the balance may tip towards a hyper-excitatory state. Although the mechanism of action isn’t entirely understood, as a GABA analogue, acamprosate may normalize the brain’s balance of excitatory and inhibitory neuronal activity. In doing so, it may lessen the post-acute withdrawal symptoms that may lead to relapse.
Complementary and Alternative Treatments
The September 2017 edition of the National Geographic magazine describes the use of Transcranial Magnetic Stimulation to help with cocaine addiction recovery.[xi]
Similarly, MHA has described Cranial Electrical Stimulation as a promising practice for substance use disorders.
- A 2009 open-label study at Phoenix House, the nation’s largest non-profit drug rehabilitation center, found that CES was well accepted by both clients and treatment staff, and that it could be easily integrated into the treatment regimen.[xii]
- Staff and clients viewed it as an alternative therapy that was similar to meditation but with the addition of small electrical stimulation, and the CES sessions were actually called the “meditation group” by clients and staff alike. This meditation group was integrated into a daily schedule along with psychoeducation, cognitive-behavioral therapy (CBT), and other therapeutic groups.
- Two additional 2006 meta-analyses by Smith demonstrated significant improvement in drug abstinence from the use of CES: 15 studies, 535 subjects, mean improvement 60% [xiii] N.b. however that the Smith monograph has not been peer-reviewed and that Dr. Smith is a consultant to the industry.
- Yoga, meditation and exercise, “soft belly” relaxation and the relaxation response, are also promising practices described in the MHA CAM guide:
http://www.mentalhealthamerica.net/sites/default/files/MHA_CAM.pdf
Counseling
Although medication-assisted treatment is much more effective than counseling or group therapy or self-help groups, recovery from substance use disorders requires some form of counseling as well.
Outpatient treatment programs are the usual setting for ongoing prescription drug abuse treatment.
Cognitive Behavioral Therapy
Cognitive behavioral therapy -- or CBT -- teaches a person how to recognize moods, thoughts, and situations that stimulate drug craving. A therapist helps the person avoid these triggers, and replace negative thoughts and feelings with healthier ones that are more consistent with sobriety.
The skills learned in cognitive behavioral therapy can last a lifetime, making it a potentially powerful method of drug abuse treatment. However, not all therapists are trained in cognitive behavioral therapy techniques, which can be complex.
Contingency Management Therapy
In contingency management therapy, a person in drug abuse treatment receives positive incentives for staying clean. Vouchers for goods and services, or privileges in a more rigid treatment setting are common incentives. Contingency management therapy is effective in drug rehab studies. But skeptics point out its high costs, and that when incentives stop, its positive effects decline.
Motivational Interviewing
Traditional therapies for drug abuse treatment involved confrontation. Addicts are masters of denial, the thinking went, and therapy should break down walls to force them to accept the reality of their addiction.
While confrontation may still have a role, many therapists instead promote motivational interviewing, a newer counseling method. In motivational interviewing, a therapist seeks to understand and enhance an addicted person's natural motivation for change. For example, if the person reveals he is motivated by love of his family, or returning to work, these may become the focus of therapy.
Couples and Family Therapy
Prescription drug abuse and opioid addiction don't only affect the user's life; the whole family is transformed. Strong relationships with family and friends are essential for successful drug abuse treatment. Various counseling methods include the spouse and other family members of the addicted person.
Maintenance Therapy
Substance use disorders are chronic, relapsing illnesses. Just like other chronic illnesses such as diabetes or high blood pressure, addiction treatment in some form must be lifelong.
Many people continue to take maintenance medication-assisted therapy. A form of buprenorphine (Probuphine) is now available as an implant under the skin for preventing a relapse of opioid dependence. It provides a constant dose of buprenorphine for six months and can be used by people who have completed acute detoxification and are already maintained on a stable dose of oral buprenorphine. Other medications include methadone, naltrexone (which blocks opiate receptors and prevents opiates from causing a high) or Suboxone (buprenorphine/naloxone) -- medications that are sometimes taken for many years in order to minimize relapse risk. By the same token, experts say, they should also continue some form of counseling.
The idea of long-term, open-ended treatment runs counter to the one-time view that a person was likely "cured" in a relatively short time after attending a drug rehab program. However, evidence is mounting that lifelong treatment with maintenance medication along with counseling or therapy should be standard drug abuse treatment for most people with relapsing substance use disorders.
Addiction Treatment Is Effective
Addiction treatment is successful in reducing substance use, illegal activity, and suicidal ideation.[xiv] The conclusion that treatment is effective is found in over 600 published scientific papers.[xv] Relapse rates for treatment of alcohol, opiates, and cocaine are less than those for hypertension and asthma, and equivalent to those of diabetes (all chronic conditions). Compliance rates for treatment of alcohol, opiates, and cocaine are greater than compliance for hypertension and asthma.[xvi]
SAMHSA concluded in 2009: “There is a great paucity of nationwide data related to the cost benefit of substance use treatment. However, the limited research in some states suggests that there is a major benefit to substance use treatment…. The benefits of treatment far outweigh the costs. Even beyond the enormous physical and psychological costs, treatment can save money by diminishing the huge financial consequences imposed on employers and taxpayers.”[xvii]
Decriminalization
Criminalization of drug use is a major barrier to getting people to initiate and accept treatment. As dramatized by Human Rights Watch,[xviii] there is a dramatic toll taken by America’s criminalization of the use and possession of illicit drugs. MHA calls upon legislators to emphasize treatment rather than punishment whenever possible to remedy this tragic and expensive policy failure. There is growing worldwide support to take the next step and eliminate criminal penalties for drug use and possession. Leading medical, public health and human rights groups have endorsed the approach, including The United Nations (UN) and the World Health Organization (WHO), the International Red Cross, the American Public Health Association, American Civil Liberties Union, the NAACP, and Latino Justice.
Of course, public drunkenness has long-since been decriminalized almost everywhere, but many communities continue to enforce “open container” and “nuisance party” laws in order to contain the disruption of the secondary phenomena of public drinking and carousing. And while many American cities and states have legalized or decriminalized cannabis use and minimal possession, while retaining prohibitions of public use, only Indiana and Oregon have proposed to reduce penalties across the board for other drugs.[xix] Drug courts[xx] and other specialized treatment courts have provided an alternative to criminal sanctions, and some help for co-occurring mental health conditions, but American society still strictly criminalizes the use and possession of many psychoactive chemicals.
California Proposition 36 (2000), the Substance Abuse and Crime Prevention Act of 2000, was an initiative that allowed qualifying defendants convicted of non-violent drug possession offenses to receive a probationary sentence in lieu of incarceration. As a condition of probation, defendants were required to participate in and complete a licensed and/or certified community drug treatment program. If the defendant failed to complete this program or violates any other term or condition of their probation, then probation could be revoked and the defendant could be required to serve an additional sentence which may include incarceration.
The University of California, Los Angeles, which was chosen to run the required evaluation of Proposition 36, issued three annual reports on the implementation and impact of the program since 2003. The 2006 UCLA study showed that Proposition 36 was saving taxpayers $2.50 for every $1 invested. It was estimated that the legislation would save $1.5 billion in five years in addition to increasing the number of licensed and substance abuse "slots" by 68%.[xxi] However, the Prop 36 (2000) funding dried up. Proposition 47 (2014) followed.
Prop 47 (2014) made most drug possession and minor nonviolent property crimes misdemeanors rather than felonies. The measure also required that money saved as a result of the measure would be spent on "school truancy and dropout prevention, victim services, mental health and drug abuse treatment, and other programs designed to keep offenders out of prison and jail." This should breathe new life into the treatment priorities of proposition 36 (2000).
Prevention
As with other behavioral health issues, Mental Health America emphasizes the need for effective prevention to avoid the many costs of treatment interventions later in the course of the condition. The 2016 Surgeon General’s 2016 report Facing Addiction in America, Appendix B, gives a comprehensive overview of evidence-based substance use disorder prevention programs, https://addiction.surgeongeneral.gov/surgeon-generals-report.pdf Specific prevention programs to deal with the opioid crisis are detailed in a 2017 consensus report of the National Academies: Pain Management and the Opioid Epidemic: Balancing Societal and Individual Benefits and Risks of Prescription Opioid Use (2017)[xxii]
Prevention is particularly important in avoiding the consequences of early substance use on the developing brain. Adolescence is the transition between childhood and adulthood. During this time, significant changes occur in the body, including rapid hormone alterations and the formation of new networks in the brain. A psychoactive drug produces an intoxicating effect by acting on one or more chemical messenger systems in a person's brain. Early alcohol use may have lasting consequences. People who begin drinking before age fifteen are four times more likely to develop alcohol use disorders at some time in their lives compared to those who have their first drink at age twenty or older.[xxiii] Early use of marijuana showed substantial effects on later incidence of substance use conditions and major depressive disorder in a NIDA funded longitudinal study of more than 700 individuals from early childhood into their late twenties.[xxiv] This is likely to be true for most psychoactive substances.
Call to Action
Mental Health America encourages its affiliates and mental health and substance use disorder stakeholders to advocate for promotion of healthy substance use and prevention of addiction and widespread availability and accessibility of mental health and substance use treatment services that are evidence- and strengths-based and fully integrated with each other and with general health services. MHA urges that states and the federal government respond to this acute social crisis with recovery-and wellness-oriented, family- and partner-supportive, consumer-driven, and culturally and linguistically competent services, by:
- Initiating community based coalitions to address promotion of healthy substance use and prevention of addiction and widespread availability and accessibility of evidence-based treatment and recovery services for substance use disorders.
- Recognizing and addressing the need for robust early detection and intervention programs.
- Building and developing core curricula, including appropriate training in mental health and substance use disorders, for the entire community.
- Advocating for the faithful and appropriate implementation and enforcement of the Paul Wellstone and Pete Domenici Mental Health Parity and Addiction Equity Act of 2008.[i]
- Promoting alternatives to the use of opioids for pain and protocols to prevent over-prescription and overuse of opioids when they are required.
- Increasing and monitoring outcomes of diversion for substance-related offenses.
In the 2017 Interim Report of the President’s Commission on Combating Drug Addiction and the Opioid Crisis, several critical recommendations were made, all of which are endorsed by MHA (see appendix for more details):
- Rapidly increase treatment capacity. Grant waiver approvals for all 50 states to quickly eliminate barriers to treatment resulting from the federal Institutes for Mental Diseases (IMD) exclusion within the Medicaid program. This will immediately open treatment to thousands of Americans in existing facilities in all 50 states.
- Mandate prescriber education initiatives with the assistance of medical and dental schools across the country to enhance prevention efforts. Mandate medical education training in opioid prescribing and risks of developing a substance use disorder by amending the Controlled Substance Act to require all Drug Enforcement Administration (DEA) registrants to take a course in proper treatment of pain. HHS should work with partners to ensure additional training opportunities, including continuing education courses for professionals.
- Immediately establish and fund a federal incentive to enhance access to Medication- Assisted Treatment (MAT). Require that all modes of MAT are offered at every licensed MAT facility and that those decisions are based on what is best for the patient. Partner with the National Institutes of Health (NIH) and the industry to facilitate testing and development of new MAT treatments.
- Provide model legislation for states to allow naloxone dispensing via standing orders, as well as requiring the prescribing of naloxone with high-risk opioid prescriptions; we must equip all law enforcement in the United States with naloxone to save lives.
- Prioritize funding and manpower to the Department of Homeland Security’s (DHS) Customs and Border Protection, the DOJ Federal Bureau of Investigation (FBI), and the DEA to quickly develop fentanyl detection sensors and disseminate them to federal, state, local, and tribal law enforcement agencies. Support federal legislation to staunch the flow of deadly synthetic opioids through the U.S. Postal Service (USPS).
- Provide federal funding and technical support to states to enhance interstate data sharing among state-based prescription drug monitoring programs (PDMPs) to better track patient-specific prescription data and support regional law enforcement in cases of controlled substance diversion. Ensure federal health care systems, including Veteran’s Hospitals, participate in state-based data sharing.
- Better align, through regulation, patient privacy laws specific to addiction, including 42 CFR Part.2, with the Health Insurance Portability and Accountability Act (HIPAA) to ensure that information about SUDs be made available to medical professionals treating and prescribing medication to a patient..
- Enforce the Mental Health Parity and Addiction Equity Act (MHPAEA) with a standardized parity compliance tool to ensure health plans cannot impose less favorable benefits for mental health and substance use diagnoses than for physical health diagnoses.
Effective Period:
This policy was approved by the Mental Health America Board of Directors on December __, 2017. It is reviewed as required by the MHA Public Policy Committee.
[i] PL 110-343
[1] (Chestnut Health Systems, Bloomington, IL 1998)
[ii] Alcohol Research Documentation; Later Printing edition (1960)
[iii] Page, P.B., "E. M. Jellinek and the Evolution of Alcohol Studies: A Critical Essay," Addiction 92(12):1619-1637 (1997)
[iv] Glazer, G., “The Irrationality of AA,” Atlantic April, 2015, https://www.theatlantic.com/magazine/archive/2015/04/the-irrationality-of-alcoholics-anonymous/386255/
[v] Miller, W.R. & Hester, R.K., Handbook of Alcoholism Treatment Approaches: Effective Alternatives, 3rd Edition (Allyn & Bacon, Boston 2003)
[vi] Dodes, L. and Dodes, Z., The Sober Truth: Debunking the Bad Science Behind 12-Step Programs and the Rehab Industry (Beacon Press, Boston 2014).
[vii] Ferri, M., Amato, L. & Davoli, M. (2006), “Alcoholics Anonymous and other 12-step Programmes for Alcohol Dependence,” http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD005032.pub2/abstract, http://www.cochrane.org/CD005032/ADDICTN_alcoholics-anonymous-aa-is-self-help-group-organised-through-an-international-organization-of-recovering-alcoholics-that-offers-emotional-support-and-a-model-of-abstinence-for-people-recovering-from-alcohol-dependence-using-a-12-step-appr
[viii] https://pubs.niaaa.nih.gov/publications/arh29-2/131-142.htm
Table 1 recovery summary: Only 25.0 percent of all U.S. adults with PPY alcohol dependence were still dependent in the past year. Another 27.3 percent were in partial remission—10.5 percent who met the criteria for alcohol abuse and 16.8 percent who reported a subclinical array of dependence symptoms. Nearly half of all people with PPY dependence met the criteria for full remission from alcohol dependence in the past year. This figure includes asymptomatic risk drinkers (11.8 percent), low-risk drinkers (17.7 percent), and abstainers (18.2 percent). Combining low-risk drinkers (NR) and abstainers (AR), more than one-third (35.9 percent) had a past-year status indicative of full recovery. Most of those classified as fully recovered reported an interval of 5 years or more since remission of dependence, resulting in an estimated stable recovery rate of 29.6 percent.
[x] There are many internet sites that discuss MAT. Among those consulted for this description, which is not original, MHA recommends https://drugabuse.com/library/medication-assisted-treatment/ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3202507/ and https://www.cabdirect.org/cabdirect/abstract/20093195682
[xi] Terraneo, A., Leggio, L., Saladini, M., Ermani, M., Bonci, A. & Gallimberti, L., “Transcranial Magnetic Stimulation of Dorsolateral Prefrontal Cortex Reduces Cocaine Use: A Pilot Study,” Eur Neuropsychopharmacol. 2016 Jan;26(1):37-44. doi: 10.1016/j.euroneuro.2015.11.011. Epub 2015 Dec 4. https://www.ncbi.nlm.nih.gov/pubmed/26655188
[xii] Deitch, D.A., Butler, J., Fisher, C.A., Hargrave, S. & John, N., “A Retrospective Chart Review of Cranial
Electrotherapy Stimulation for Clients Newly Admitted to Residential Drug Treatment,” unpublished,
http://www.fisherwallace.com/uploads/Phoenix_House_Pilot_Summary-November_2009.pdf
[xiii] Smith, R.B., “A Summary Look at Studies of Cranial Electrotherapy Stimulation: Its First Fifty Years, Plus Three” (monograph), published by Tate Publishing & Enterprises, Mustang, Oklahoma (2006). Available on line at
http://www.fisherwallace.com/published-research-on-cranial-electrotherapy-stimulation
[xiv] NIH/NIDA, Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition), https://www.drugabuse.gov/publications/principles-drug-addiction-treatment-research-based-guide-third-edition/frequently-asked-questions/how-effective-drug-addiction-treatment
[xv] O’Brien, C.P. & McLellan, A.T., “Myths about the Treatment of Addiction,” The Lancet 347: 237-240 (1996).
[xvi] Id.
[xviii] https://www.hrw.org/report/2016/10/12/every-25-seconds/human-toll-criminalizing-drug-use-united-states
[xix] Under Oregon House Bill 2355 (2017), drugs like LSD, MDMA, cocaine, meth, oxycodone, and heroin are essentially decriminalized in small amounts. Each drug listed is accompanied by the following text, indicating possession is only a felony if: “(a) The person possesses a usable quantity of the controlled substance and: (A) At the time of the possession, the person has a prior felony conviction; (B) At the time of the possession, the person has two or more prior convictions for unlawful possession of a usable quantity of a controlled substance.” The “misdemeanor” title applies for varying amounts of different drugs. For example, the maximum allowable amount of acid is up to “40 units,” while individuals may have up to five MDMA pills or less than one gram before their “offense” crosses the line into a felony. Less than two grams of cocaine constitutes a misdemeanor. In Indiana, HEA 1006-2015 reduced sentencing for drug crimes and simultaneously provided for treatment in lieu of incarceration. A recidivism evaluation was required by the legislation, and after the first year, the numbers look very promising.
[xx] A drug defendant who agrees to drug court spends roughly 12 to 15 months attending treatment sessions and undergoing random drug tests while appearing before the drug court judge on a regular basis. Those who fail to appear in court or fail drug tests are arrested and often given a brief jail sentence. Those who succeed usually get their charge dismissed. See also MHA Position Statement 53, Mental Health Courts, http://www.mentalhealthamerica.net/positions/mental-health-courts
[xxi] Evaluation of the Substance Abuse and Crime Prevention Act 2002 Report (2003) https://s3.amazonaws.com/academia.edu.documents/44827407/Evaluation_of_the_Substance_
Abuse_and_Crime_Prevention_Act_2002_Report.pdf?AWSAccessKeyId=AKIAIWOWYYGZ2Y53UL3A&Expires=1504312228&Signature=
BdnXCO7OEx%2B94Efi%2Bn6r194fQSc%3D&response-content-disposition=inline%3B%20filename%3DEvaluation_of_the_Substance_Abuse_and_Cr.pdf
[xxii] https://www.nap.edu/catalog/24781/pain-management-and-the-opioid-epidemic-balancing-societal-and-individual?utm_source=NASEM+News+and+Publications
&utm_campaign=dc30f50fb6-NAP_mail_new_2017-10-02&utm_medium=email&utm_term=0_96101de015-dc30f50fb6-103386193&goal=0_96101de015-dc30f50fb6-103386193
&mc_cid=dc30f50fb6&mc_eid=b175279007
[xxiii] Id.
[xxiv] Schlabige, J., "Early Use of Drugs May Lead to Later Psychiatric Disorders,” NIDA Notes, Vol.18, No. 5 (2003).
[ii] U.S. Department of Health and Human Services (HHS), Office of the Surgeon General, Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Washington, DC: HHS, November 2016, at p. 2-22 and 2-23. https://addiction.surgeongeneral.gov/sites/default/files/surgeon-generals-report.pdf
[v] New Freedom Commission on Mental Health, Achieving the Promise: Transforming Mental Health Care in America/Final Report. DHHS Pub. No. SMA-03-3832. Rockville, MD: 2003, monograph available for download at http://store.samhsa.gov/product/Achieving-the-Promise-Transforming-Mental-Health-Care-in-America-Executive-Summary/SMA03-3831
[vi] U.S. Department of Health and Human Services (HHS), Office of the Surgeon General, Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Washington, DC: HHS, November 2016. https://addiction.surgeongeneral.gov/sites/default/files/surgeon-generals-report.pdf
[vii] Id., Introduction of Kana Enomoto.
[viii] The next sections are derived from https://www.samhsa.gov/disorders/substance-use
[ix] Substance Abuse and Mental Health Services Administration, Center for Behavioral Health Statistics and Quality, Rockville, MD. The NSDUH Report: Adults With Mental Illness or Substance Use Disorder Account for 40 Percent of All Cigarettes Smoked [PDF–563 KB], (March 20, 2013), https://www.samhsa.gov/data/sites/default/files/spot104-cigarettes-mental-illness-substance-use-disorder/spot104-cigarettes-mental-illness-substance-use-disorder.pdf .
[x] Centers for Disease Control and Prevention. Vital Signs: Current Cigarette Smoking Among Adults Aged ≥18 Years With Mental Illness—United States, 2009–2011. Morbidity and Mortality Weekly Report 2013; 62(05): 81-7, https://www.cdc.gov/mmwr/preview/mmwrhtml/mm6205a2.htm
[xi] McArdle, P.A., “Cannabis Use by Children and Young People,” Arch Dis Child 91(8): 692–695 (2006).
doi: 10.1136/adc.2005.071860, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2083022/
[xiii] http://www.webmd.com/mental-health/news/20170113/hallucinogens-future-of-mental-health-treatment#1
[xiv] U.S. Department of Health and Human Services (HHS), Office of the Surgeon General, Facing Addiction in America: The Surgeon General’s Report on Alcohol, Drugs, and Health. Washington, DC: HHS, November 2016, at p. 1-8 . https://addiction.surgeongeneral.gov/sites/default/files/surgeon-generals-report.pdf
[xv] Center for Behavioral Health Statistics and Quality. (2016). Key substance use and mental health indicators in the United States: Results from the 2015 National Survey on Drug Use and Health (HHS Publication No. SMA 16-4984, NSDUH Series H-51). Retrieved from http://www.samhsa.gov/data/



this page