You are here
Position Statement 45: Discipline and Positive Behavior Support in Schools
Policy
As a leading advocate for the mental health and wellness of children and adolescents, Mental Health America (MHA) opposes corporal punishment[1] and zero tolerance policies. MHA supports individuated school disciplinary processes that take account of mental health conditions and emotional disturbances and promote the healthy mental and emotional development of our country's youth.[2] More proactively, MHA supports evidence-based school-wide positive behavior support and “no reject, no eject” policies aimed at providing a child who misbehaves with the necessary resources to promote behavior change in positive, non-punitive ways.
Background
Corporal punishment involves the deliberate infliction of pain upon a child, by an adult, to correct and/or punish the child's perceived misbehavior. Scientific research has concluded that corporal punishment is ineffective and detrimental to the emotional and educational needs of children.[3] There are many more effective means of discipline which promote self-control and the development of appropriate socially adaptive behaviors in constructive, non-harmful ways.
Many other school disciplinary measures, while less physically violent, are often equally harsh and damaging to the educational and social fabric of the school and lead to students with mental health needs being ignored, or worse, dropping out of school. Thus, the widespread use of suspension and expulsion for often minor infractions that is the hallmark of zero tolerance policies has compromised the appropriate role of schools in shaping appropriate student behavior.[4]
A “zero tolerance policy” is a school or district policy that mandates predetermined consequences or punishments for specific offenses that are intended to be applied regardless of the seriousness of the behavior, mitigating circumstances, or situational context.[5] MHA believes that zero tolerance policies are authoritarian, ineffective,[6] and contrary to common sense. MHA is also concerned that zero tolerance policies use broad and vague definitions of offenses and result in inconsistent and sometimes overzealous application of consequences, especially as they relate to students from diverse racial, ethnic and economic backgrounds.[7]
But MHA’s central objection is the effect of rigid zero tolerance policies on students with unmet mental health and emotional needs. Fair treatment for students with mental health conditions or emotional disturbances requires individuated consideration of all the circumstances of an alleged offence and reasonable accommodation of each person’s needs, including access to mental health services, and all interventions, including discipline, should be geared toward ensuring the student’s future academic and social success.
It is clear from national data that zero tolerance policies, and the suspensions that often result from them, disproportionately affect children with disabilities:
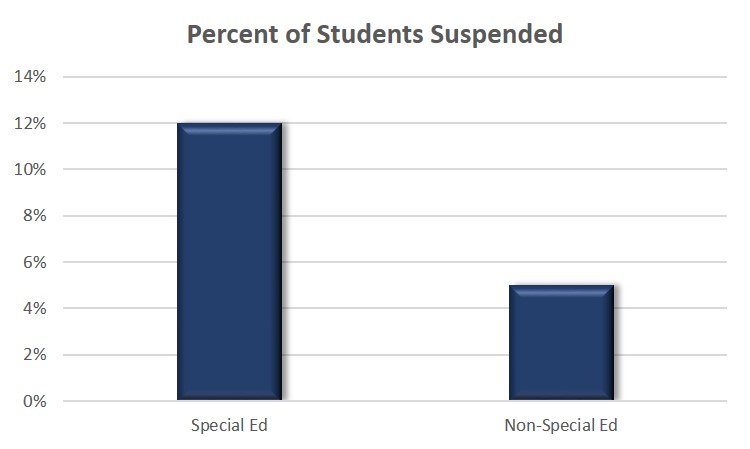
http://www2.ed.gov/about/offices/list/ocr/docs/2013-14-first-look.pdf
Thus, it is imperative that traditional school disciplinary procedures be replaced with positive classroom-management approaches are empirically-validated to improve the academic as well as the social success of all students, and especially those students with behavioral health concerns.
The result of more than 700 interviews spanning three years, the 2014 Council of State Governments (CSG) Justice Center’s School Discipline Consensus Report reflects a consensus among a wide collection of leaders in the areas of education, health, law enforcement and juvenile justice, establishing what it will take to reduce the number of youth suspended from school while providing learning conditions that help all students succeed:
Research and data on school discipline practices are clear: millions of students are being removed from their classrooms each year, mostly in middle and high schools, and overwhelmingly for minor misconduct. When suspended, these students are at a significantly higher risk of falling behind academically, dropping out of school, and coming into contact with the juvenile justice system. A disproportionately large percentage of disciplined students are youth of color, students with disabilities, and youth who identify as lesbian, gay, bisexual, or transgender (LGBT[Q]).
Anyone who wants to make students feel safer in school, improve high school graduation rates, and close the achievement gap needs to have a plan to reduce the number of youth who are suspended from school,” said Michael Thompson, director of the CSG Justice Center. “This report provides that roadmap, and it is endorsed by a broad spectrum of interest groups that have a significant stake in this issue.
The Consensus Report condemns zero tolerance and offers a wide range of recommendations, focusing on expectations for student behavior instead of a system of punishments, limiting the role of law enforcement officials in classroom management and targeting students who are at-risk for discipline issues and taking steps to intervene early, before serious offenses occur.[8]
The Consensus Report was the culmination of a long process of study that looked at the school environment rather than the individual offence as the proper focus of discipline. Thus, as early as 2004, the American Academy of Pediatrics published a policy calling for universal school-based programs to encourage mental health and prevent mental illness:
Activities …need to be ubiquitous so that they target all children in all school settings. Preventive programs are those that focus on decreasing risk factors and building resilience, including providing a positive, friendly, and open social environment at school and ensuring that each student has access to community and family supports that are associated with healthy emotional development. A sense of student “connectedness” to schools has been found to have positive effects on academic achievement and to decrease risky behaviors. For example, schools should provide students with multiple and varied curricular and extracurricular activities, thereby increasing the chances that each student will feel successful in some aspect of school life. Schools also should provide numerous opportunities for positive individual interactions with adults at school so that each student has positive adult role models and opportunities to develop a healthy adult relationship outside his or her family. Schools can provide families with support services and should implement “prevention” curricula (e.g., curricula that decrease risk-taking behaviors). Behavioral expectations, rules, and discipline plans should be well publicized and enforced school-wide.[9]
Similarly, during 2004-2006, the Task Force on Community Preventive Services (Task Force) of the United States Center for Disease Control conducted a systematic review of published scientific evidence concerning the effectiveness of these programs. The review provided strong evidence that universal school-based programs decrease rates of violence and aggressive behavior among school-aged children. Program effects were demonstrated at all grade levels. An independent meta-analysis confirmed and supplemented these findings. Based on strong evidence of effectiveness, the Task Force recommended the use of universal school-based programs to prevent or reduce violent behavior.[10]
There are a number of evidence-based interventions that have been developed and tested over the past several decades that can replace traditional disciplinary procedures to promote children’s mental health. These interventions are sometimes referred to as mental health promotion, social and emotional learning, and school climate interventions, and target different aspects of the classroom experience through varying theories of change, but all share the goal of fostering resilience and positive mental health among teachers and students.
Good Behavior Game (GBG). GBG is a universal classroom prevention strategy of behavior management that centers on positive reinforcement. Teachers use GBG to help students develop skills such as teamwork and self-regulation[11]. GBG is integrated into the school day, including instructional time, transition times, and lunch as a team-based competition in which everyone can win. Teachers give teams positive reinforcement for meeting behavioral expectations, monitoring and managing their own behaviors and supporting the positive behavior of peers. GBG has been demonstrated to reduce aggressive, disruptive and off-task behavior in elementary school males, reduce smoking and use of mental health services in middle school males, and reduce alcohol use, tobacco use, illicit drug use and suicide attempts in young adult males (ages 19 to 21), along with increase high school graduation rates. A Washington State Institute for Public Policy cost-benefit analysis of implementing the GBG estimated for every dollar spent on GBG, there are $64.18 in societal benefits.[12]
4Rs. The 4Rs program (Reading, Writing, Respect & Resolution) provides a curriculum for integrating SEL and language arts into Pre-K to middle school classrooms.[13] Teachers follow a grade-specific curriculum that moves from Read Aloud lessons for younger audiences to Book Talks that encourage discussion and role-playing to Applied Learning where students practice skills related to a specific theme. The 4Rs also includes parental activities for children to participate in at home. The 4Rs program has been shown to lower teacher-reported aggression levels and lead to fewer student depression symptoms, decreased attention and hyperactivity problems, and increased social competency.[14] Among those with the greatest behavioral risk, evaluations show significant improvements in attendance, academic skills, and standardized testing scores. A study by the Center for Benefit-Cost Studies in Education found that for every $1 investment in the 4Rs program, $11 of economic benefit is delivered.[15]
Promoting Alternative Thinking Strategies (PATHS). The PATHS program is an SEL curriculum designed for Pre-K through elementary students.[16] The program is based on evidence that children experience and react to emotions before they develop cognitive abilities to verbalize them. PATHS includes five SEL domains: self-control, emotional understanding, positive self-esteem, relationships, and interpersonal problem-solving skills. Each lesson is approximately 30 minutes and is incorporated into the classroom two to three times a week. At-home activities supplement classroom instruction. Research demonstrates reductions in teacher reported aggressive behavior, behavior problems, and depression and sadness among students. Improvements in students’ self-control, vocabulary for emotion, standardized test scores, cognitive skills, ability to tolerate frustration and use conflict resolution strategies, and classroom behavior and engagement were also documented.[17] A Washington State Institute for Public Policy cost-benefit analysis found for every dollar spent on PATHS, there are $21.24 in societal benefits.[18]
School-Wide Positive Behavioral Interventions & Supports (SWPBIS). Unlike the previously described programs, PBIS is not a packaged curriculum or intervention, but rather a framework for assisting schools in integrating behavioral interventions that enhance academic and social behavior outcomes. Research indicates that SWPBIS contributes to decreased classroom disruptions and office discipline referrals, increased academic achievement and performance, and improved school climate and safety.[19] According to a Washington State Institute for Public Policy cost-benefit analysis, for every dollar spent on SWPBIS, there are $13.49 in societal benefits.[20]
SWPBIS has been the focus of federal efforts, and has come to refer to both that specific intervention and others that support positive behaviors in schools.[21] For convenience SWPBIS will be referred to throughout under this more general lens. SWPBIS is based on the assumption that when faculty and staff in a school actively teach and acknowledge expected behavior, the proportion of students with serious behavior problems will be reduced and the school’s overall climate will improve.[22] Strategies such as behavioral coaching, behavioral rehearsal and role play, daily goal setting, and self-monitoring can be helpful in teaching students to manage their own behavior and emotions more effectively. Skill building may be an important intervention for students who are displaying aggressive and disruptive behaviors. A concerted effort is made to gain an understanding of the underlying causes for disruptive behavior and to teach alternative behavioral strategies.
A Technical Assistance Center on Positive Behavioral Interventions and Supports has been established by the Office of Special Education Programs, U.S. Department of Education. http://www.pbis.org/default.aspx. Noting that as of 2016, more than 23,000 schools across the nation had adopted this approach, the website defines SWPBIS as follows:
One of the foremost advances in school-wide discipline is the emphasis on school-wide systems of support that include proactive strategies for defining, teaching, and supporting appropriate student behaviors to create positive school environments. Instead of using a piecemeal approach of individual behavioral management plans, a continuum of positive behavior support for all students within a school is implemented in areas including the classroom and non-classroom settings (such as hallways, buses, and restrooms). Positive behavior support is an application of a behaviorally-based systems approach to enhance the capacity of schools, families, and communities to design effective environments that improve the link between research-validated practices and the environments in which teaching and learning occurs. Attention is focused on creating and sustaining primary (school-wide), secondary (classroom), and tertiary (individual) systems of support that improve lifestyle results (personal, health, social, family, work, recreation) for all children and youth by making targeted behaviors less effective, efficient, and relevant, and desired behavior more functional….SWPBIS is a systems approach to establishing the social culture and behavioral supports needed for all children in a school to achieve both social and academic success. PBIS is not a packaged curriculum, but an approach that defines core elements that can be achieved through a variety of strategies.
The Department of Education website compiles the evidence base for SWPBIS.[23]
On August 4, 2016, the U.S. Department of Education’s Office of Special Education and Rehabilitative Services (OSERS) issued guidance that emphasizes the requirement that schools provide positive behavioral supports to students with disabilities who need them. It also clarifies that the repeated use of disciplinary actions may suggest that children with disabilities may not be receiving appropriate behavioral interventions and supports. When schools fail to consider and provide for needed behavioral supports through the Individualized Education Program, it is likely to result in children not receiving the free appropriate public education to which they are entitled under federal law:
All students, including those with disabilities, should have the supports and equitable educational opportunities they need to be successful in school,” said U.S. Secretary of Education John B. King Jr. “It’s our duty as parents and educators to ensure that children who show up at school to learn get the maximum out of their educational experience. This guidance will help schools create a safe, supportive learning environment for those students who need additional behavioral supports and services to help them thrive.[24]
The success of positive behavioral support approaches should be assessed through school climate and school connectedness surveys. The Department of Education defines school climate as “a broad, multifaceted concept that involves many aspects of the student’s educational experience. A positive school climate is the product of a school’s attention to fostering safety; promoting a supportive academic, disciplinary, and physical environment; and encouraging and maintaining respectful, trusting, and caring relationships throughout the school community no matter the setting—from Pre-K/Elementary School to higher education.”[25] In 2016 the Department of Education released a series of school climate surveys, noting that “measuring school climate is critical for improving school climate because high quality school climate data allow you to understand the perceptions of the students, staff, and parents in your school or district; monitor progress; make data-driven decisions; involve stakeholders; and adapt to shifting needs related to school climate.”[26] To this end, the survey measures the following domains:
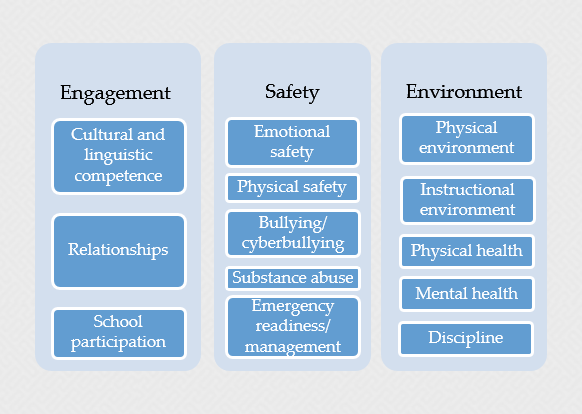
https://safesupportivelearning.ed.gov/edscls/measures
Positive behavioral supports should be situated inside of a larger school-wide and community-wide orientation toward promoting mental health. In the school, other evidence-based programs like 4 R’s integrate aspects of social and emotional learning into reading curriculums to reinforce the skills taught by positive behavioral supports.[27] Parents, pediatricians, and other members of the community should also be engaged in reinforcing healthy social and emotional development. In 2016, Mental Health America, Trust for America’s Health, and the Healthy Schools Campaign convened a panel of experts to determine a set of policy recommendations to accomplish these goals. A recent blog authored by MHA staff reported on the work of the National Collaborative on Education and Health in highlighting and integrating the school programs that have produced the most impressive results under a number of different names—such as social and emotional learning, mindsets, school climate, and trauma-informed schools.[28]
Mental Health America believes that universal positive supports should be a part of training for each adult in the school and seen as a crucial part of their role in creating a safe and healthy school climate. For example, the Dean of the education school at the College of Saint Elizabeth has mainstreamed evidence-based social and emotional skills into the teacher curriculum, and co-directs the School Culture and Climate Initiative to transmit these same ideas to local schools. In partnership with Rutgers, the evidence-based learning modules have been made available online for teachers.[29]
Further, health care should coordinate with education to share expertise and provide necessary supports to make school-wide interventions a success. While we see early examples, the federal government should lend robust policy support. Nationwide Children’s Hospital, for example, noted that in its program, Partners for Kids (PFK), “a major expense … was the cost of behavioral health drugs, which made up one-third of all the pharmacy costs for the children PFK covered, many of whom came from inner-city, low-income areas and were being treated in emergency rooms. To reduce the costs of treating such children for behavioral problems, PFK focused on preventing problems with such evidence-based initiatives as the Good Behavior Game, The Incredible Years®, Safer Choices, and home visiting with the Supporting Partnerships to Assure Ready Kids (SPARK).
Unfortunately, universal school-based prevention is still typically “grant-based, and often unpredictable or unsustainable.”[30] But developments in California show positive options on the horizon. A recent concept paper directed at implementing California’s innovative mental health prevention set-aside legislation[31] focused on a proposed state-wide Response to Intervention (RTI) approach: “decoupling the ‘emotionally disturbed’ eligibility and/or psychiatric diagnosis from the provision of services through endorsing and implementing a tiered approach to prevention and intervention targeted toward salient risk factors students may possess regarding life adjustments, transitions, adverse childhood experiences, and emotional/behavioral concerns. Prevention is understood to be the foundation of the approach, with addressing risks to students’ emotional/behavioral health being the initial focus of intervention, versus waiting for actual functional deficits and psychiatric pathologies to develop. RTI ‘provides the opportunity to help struggling children immediately rather than waiting until well-ingrained patterns of emotional and behavioral difficulties are established.’”[32]
The National Center for Learning Disabilities sponsors the Response to Intervention Action Network, which has compiled a helpful compendium of field studies of RTI programs around the country.[33] While the studies are small and focused on elementary education, and secondary education remains to be studied, the authors concluded that: “All of the studies examining the impact of an RTI program on academic achievement or performance resulted in some level of improvement, and the authors attributed the changes to the RTI approach they used. Thus, there is emerging evidence that a tiered early intervention approach can improve the academic performance of at-risk students.”[34]
Mental Health America has consistently supported efforts in Congress and the states to put more funding and emphasis on behavioral health supports in schools and on more specific interventions like school-based mediation and mental health programs, anti-bullying programs that integrate school-wide positive behavior support and redefine the bullying construct, confidential peer support and counseling and intervention programs for children in crisis, related teacher training and evaluation, and broadening mental health support beyond special education programs to deal with a wider range of mental health conditions and emotional disturbances.
The key word is support, not therapy, and the goal of SWPBIS and all programs that focus on positive behavioral interventions and supports is avoidance of discrimination by making mental wellness a central concern of all schools and for all students, while constantly screening and referring students for interventions that respond to problems as they develop.
Mental Health America is on record in support of “no reject, no eject” policies that deal with the underlying issues related to misbehavior and focus on success and connectedness rather than getting rid of challenging students through suspension or expulsion. MHA believes that it is always preferable not to deprive students of educational services to which they are entitled by law and to integrate all students into the classroom whenever possible, using more subtle tools that shape better behavior rather than giving up or isolating a student when the student acts out.
Call to Action
· MHA strongly supports the application of disciplinary actions and policies that promote the health and well-being of students. In particular, MHA supports school-wide positive behavior support and “no reject, no eject” policies aimed at providing a child with a mental health condition or a serious emotional disturbance with the necessary supports and resources that support behavior change in positive, non-punitive ways.
· These policies should comply with the letter and spirit of the Individuals with Disabilities Education Act (IDEA) and provide that no student be suspended or expelled prior to a manifestation determination that the behavior in which a child is engaged is not related to his or her disability; otherwise, students should be dealt with in an individuated way that is appropriate for their age, sex, mental health condition, emotional development, and special educational needs and the misbehavior committed.
· Concretely, this means that advocates and MHA affiliates should sponsor and support legislation and policy changes that narrowly tailor rigid zero tolerance policies and replace them with required consideration of individual mental health and emotional conditions and early, equal and effective access to comprehensive mental health services.
· In addition, advocates and affiliates should demand that schools and school districts liberally construe their obligations under the Individuals with Disabilities Education Act, the Americans with Disabilities Act of 1990 and Section 504 of the Rehabilitation Act of 1973 to preclude the application of zero tolerance policies in cases where a mental health condition or a serious emotional disturbance allows or requires a reasonable accommodation.
- In §504, the focus is on non-discrimination. As applied to the schools, the language prohibits the denial of public education participation or enjoyment of the benefits offered by public school programs because of a child’s disability. Congress conditioned future receipt of federal funds on a district’s compliance with these requirements. Thus, advocates should threaten federal intervention if the implementation of a zero-tolerance policy threatens educational access for a child with a disability.
- The Americans with Disabilities Act (“ADA”) picks up where the Rehabilitation Act left off. Borrowing from the §504 definition of disabled person, the ADA applied those standards to most private sector businesses, including private schools. The passage of the ADA does nothing to change a public school’s or school district’s obligations to provide educational services to its disabled students under the IDEA. The courts have interpreted §504 and the ADA almost identically, applying doctrines and interpretations freely between the two laws.
· MHA will support school-wide positive behavior support legislation in the Congress. MHA will provide information to the affiliate field and others to promote State and local legislation which transforms school discipline into a system of supports that furthers behavioral health.
- The implementation of education-related regulations and programs should be coordinated with health regulations and programs. For example, The Every Student Succeeds Act implementation should include consideration of Medicaid and other federal health programs and vice-versa, since the spending in each of these programs influences the other. New opportunities include the Medicaid free care policy change, the preventive services rule change and broadening definitions of Medicaid behavioral health services,[35] which provide opportunities for additional reimbursement for mental health services in school. These opportunities should be further leveraged to spread scale a range of delivery models for mental health services in schools and early care and education.
· Stronger incentives should be put in place for healthcare systems to partner with schools and early care and education, and promote mental health inside and outside the healthcare setting. This includes more robust evaluation of value-based payment models to determine their utility in enabling healthcare systems and payers to financially support social and emotional learning in education settings (e.g., Trillium Community Health Plan in Oregon funds the Good Behavior Game in schools).
· Federal and state policies should support expansion of the number of school counselors and other mental health personnel in education settings, as well as additional staffing in early care and education to address behavioral health concerns. Needs assessments should assess workforce needs and capacity. The Civil Rights Data Collection (CRDC) survey will begin collecting data on access to instructional aides, support services staff, psychologists, social workers, nurses, and school administrators from every school for the 2015-2016 CRDC, presenting an opportunity to identify gaps in school staffing. Expanding the workforce – such as through partnerships with community colleges to train paraprofessionals and, where appropriate, recruiting parents and other community members to co-administer certain programs – can also help address shortages.
· ESSA report cards and state plan non-academic measures, and other policies such as the recent Head Start regulations, should incorporate measures of school climate and connectedness among all individuals in a school setting.
- Healthcare outcome measurements and education reporting requirements should have common indicators (e.g., kindergarten readiness, third grade reading levels or absenteeism) to reinforce the benefit that efforts in each sector have in the other. Data should be shared and integrated between health and education to track these measures, identify the priority issues and implement evidence-based interventions in response.
Effective PeriodThe Mental Health America Board of Directors approved this policy on December 3, 2016. It will be reviewed as required by the Public Policy Committee.Expiration: December 31, 2021 |
[1] The abolishment of corporal punishment in our nation's schools is also called for by, inter alia, the National PTA, the American Academy of Pediatrics, the American Academy of Child and Adolescent Psychiatry, the National Congress of Parents and Teachers, the National Education Association, the American Bar Association, and EPOCH-USA.
[2] Flaherty, L. & Osher, D., “History of Mental Health in Schools in the United States,” in M.D. Weist, S. Evans, & N. Tashman (Eds.), School Mental Health Handbook (pp.11-22). New York: Kluwer Academic Publishing Company (2002).
[3] See, e.g., American Psychological Association press release, dated June 26, 2002: “In a large-scale meta-analysis of 88 studies, psychologist Elizabeth Thompson Gershoff, PhD, of the National Center for Children in Poverty at Columbia University, looked at both positive and negative behaviors in children that were associated with corporal punishment. Her research and commentaries on her work are published in the July 2002 issue of Psychological Bulletin, published by the American Psychological Association.”
While conducting the meta-analysis, which included 62 years of collected data, Gershoff looked for associations between parental use of corporal punishment and 11 child behaviors and experiences, including several in childhood (immediate compliance, moral internalization, quality of relationship with parent, and physical abuse from that parent), three in both childhood and adulthood (mental health, aggression, and criminal or antisocial behavior) and one in adulthood alone (abuse of own children or spouse). Gershoff found "strong associations" between corporal punishment and all eleven child behaviors and experiences. Ten of the associations were negative such as with increased child aggression and antisocial behavior. The single desirable association was between corporal punishment and increased immediate compliance on the part of the child.” http://www.apa.org/releases/spanking.html
[4] Writing in the Harvard Education Review, Pedro Noguera argues persuasively that the primary function of harsh punishment is to assert authority rather than to change behavior. Pedro A. Noguera, “Preventing and Producing Violence: A Critical Analysis of Responses to School Violence,” Harvard Education Review (1995), p. 189-212.
[5] American Psychological Association, Zero Tolerance Task Force Report, “Are Zero Tolerance Policies Effective in the Schools? An Evidentiary Review and Recommendations American Psychologist 63(9):852-62 (2006), http://www.apa.org/releases/ZTTFReportBODRevisions5-15.pdf., http://www.apa.org/pubs/info/reports/zero-tolerance.pdf .
[6]Skiba, R.J. & Knesting, K., "Zero Tolerance, Zero Evidence: An Analysis of School Disciplinary Practices," Indiana Education Policy Center (2000), New Dir Youth Dev. 92:17-43 (2001), http://www.dignityinschools.org/content/history-and-critique-effectiveness-zero-tolerance-discipline
[7] Id., p. 6-7
[8] Morgan, E., Salomon, N., Plotkin, M., and Cohen, R., The School Discipline Consensus Report: Strategies from the Field to Keep Students Engaged in School and Out of the Juvenile Justice System (New York: The Council of State Governments Justice Center, 2014), http://csgjusticecenter.org/youth/school-discipline-consensus-report/
[9] American Academy of Pediatrics, “School-based Mental Health Services,” Pediatrics124(2):845 (2004), http://pediatrics.aappublications.org/content/113/6/1839.full.html .
[10] Hahn, R., Fuqua-Whitley, D., Wethington, H., Lowy, J., Liberman, A., Crosby, A., Fullilove, M., Johnson, R., Moscicki, E., Price, L., Snyder, S.R., Tuma, F., Cory, S., Stone, G.,,Mukhopadhaya, K., Chattopadhyay, S., & Dahlberg, L., “The Effectiveness of Universal School-based Programs for the Prevention of Violent and Aggressive Behavior: a Report on Recommendations of the Task Force on Community Preventive Services,” MMWR Recomm Rep. 10:56(RR-7):1-12 (2007).
[12] Washington State Institute for Public Policy. Good Behavior Game. Olympia, WA: Washington State Institute for Public Policy. http://www.wsipp.wa.gov/BenefitCost/ProgramPdf/82/Good-Behavior-Game
[13] Morningside Center for Teaching Social Responsibility. The 4Rs Program. New York, NY: Morningside Center for Teaching Social Responsibility, n.d. http://www.morningsidecenter.org/4rs-program
[14] Morningside Center for Teaching Social Responsibility. 4Rs Research Study. New York, NY: Morningside Center for Teaching Social Responsibility, n.d http://www.morningsidecenter.org/4rs-research-study
[15] Belfield C et al. The Economic Value of Social and Emotional Learning. New York, NY: Center for Benefit-Cost Studies in Education, 2015. http://blogs.edweek.org/edweek/rulesforengagement/SEL-Revised.pdf
[16] Channing Bete Company. How the PATHS Program Works. South Deerfield, MA: Channing Bete Company, n.d. http://www.channing-bete.com/prevention-programs/paths/overview.html
[17] Channing Bete Company. PATHS Program Results. South Deerfield, MA: Channing Bete Company, n.d. http://www.channing-bete.com/prevention-programs/paths/results-recognition.html
[18] Washington State Institute for Public Policy. Promoting Alternative Thinking Strategies (PATHS). Olympia, WA: Washington State Institute for Public Policy. http://www.wsipp.wa.gov/BenefitCost/ProgramPdf/94/Promoting-Alternative-Thinking-Strategies-PATHS
[19] KOI Education. What is Positive Behavioral Intervention and Support? Phoenix, AZ: KOI Education, n.d. http://www.koi-education.com/pbis/
[20] Washington State Institute for Public Policy. Other School Wide Positive Behavior Programs. Olympia, WA: Washington State Institute for Public Policy. http://www.wsipp.wa.gov/BenefitCost/ProgramPdf/540/Other-school-wide-positive-behavior-programs
[21] Osher, D., Dwyer, K., & Jackson, S. (2004). Safe,Supportive, and Successful Schools: Step by Step. Longmont, CO: Sopris West (2004); Doll, B., Zucker, S., & Brehm, K., Resilient Classrooms: Creating Healthy Environments for Learning. New York: Guilford Press (2004).
[22] Colvin, Kame’enui, & Sugai, 1993; Sugai & Horner, 1994; Sugai, Sprague, Horner, & Walker, 2000.
[23] Horner, R.H., Sugai, G. & Lewis, T., “Is School-wide Positive Behavior Support an Evidence-based Practice,” (2015), published online by The Technical Assistance Center on Positive Behavioral Interventions and Supports established by the U.S. Department of Education's Office of Special Education Programs (OSEP), http://www.pbis.org/research
[24] http://www.ed.gov/news/press-releases/us-department-education-releases-guidance-schools-ensuring-equity-and-providing-behavioral-supports-students-disabilities
[28] Counts, N., and Gionfriddo, P., “New Initiative Explores the Intersection of Education and Mental Health,” Health Affairs, August 2016 (http://healthaffairs.org/blog/2016/08/23/new-initiative-explores-the-intersection-of-education-and-mental-health/)
[30] School Mental Health Comprehensive Strategy Based on RTI (California Council of Community Behavioral Health Agencies, 2015), at 4.
[31] California Mental Health Services Act Prevention and Early Intervention Program, California Welfare and Institutions Code, Division 5, Part 3.6, Section 5840.
[32] Op. cit. endnote 10, at 4-5 (citing Gresham, 2007 at 216).
[33] Hughes, C., and Dexter, D.D., “Field Studies of RTI Programs, Revised,” published on line, http://www.rtinetwork.org/learn/research/field-studies-rti-programs
[34] Id.



this page